
A pathologist's perspective (part 2 of 3)
Dr Clare Craig on damage from the so-called covid vaccines

This is part 2 of a series of three posts featuring a recent podcast with pathologist Dr Clare Craig, who is among those best placed to speak about the covid era from an evidence-based perspective. The interviewer is Will Coleshill — freedom journalist and founder/editor of Resistance GB.1
Part 1 featured introductory comments on the alternative media and medical ethics, followed by a wide-ranging discussion of the damage caused during the covid era — but not damage from the so-called covid vaccines, which is the subject of this post.
Topics covered include: the context for the rollout of the injections; early observations; the immune system soon after injection; problems in cells throughout the body; problems with regulators; how many people have died from the injections; and how many people became sick after being injected.
Again, if you want a shorter version, just read the parts in bold.
The so-called covid vaccines
[37:08]
The context
[Coleshill] What is the situation with these jabs? What makes them so dangerous?
[Craig] First of all, let’s go back to what we were saying about the treatment [the discussion in part 1 of this series]…
If you’re very sick, you need need a treatment… We ought to be treating people even if there’s a drug that we don’t know everything about… The situation is different if you’re sick.
If you’re healthy, you shouldn’t be taking [medicinal] drugs, because no drug is absolutely safe. Every time you are adding a chemical into a body that’s already functioning you are risking doing more harm than good.
[And] that ethical principle that you take a different approach in the healthy and the sick got lost somewhere along the line [during the covid era]…
Then you’ve got the situation that in America… They legally couldn’t have an emergency vaccine if there were treatments that would work. And so you’ve now got a motivation for demonising all of these treatments that were clearly working.
There is evidence in part 1, particularly in the sections on hydroxychloroquine and ivermectin, which points to viable treatments for covid being ruthlessly suppressed.
[Craig] And you’ve also got, as a result of all those policy-induced deaths when we were in 2020, a lot of people [who] honestly believed that their lives were at risk. So you’ve got huge amounts of fear propaganda, a big number of deaths on a tally and the government going hell for leather saying the only way out are these vaccines. And that created what was really a cult-like atmosphere, where people were looking to the vaccines as a saviour… [as if] that was the only thing they could do to save their lives and to get out of this awful situation.
The notion of “vaccines as a saviour” reminds me of the multiple ways in which the covid era bore more than a passing resemblance to a form of religion:

There were certainly plenty of UK church leaders embracing the vaccine saviour narrative:

[Craig] And it was really dark, all of that… really really, dark.
[Coleshill] Well you look at mass formation psychosis throughout history… the state of fear…
[Craig] Yes… we lived through it… we were all there. It was horrible.
Anyway, so the vaccines, having been presented as this saviour, were originally intended… If you read what people were saying in the positions of power back in 2020 about [the vaccines]… there was so much caution…
They were saying, “We’re going to do it for those who are at risk. Obviously it’s not going to be for anyone under the age of 50. Obviously we’re never going to give it to children… they’re not at risk… We don’t know everything about them… they’re new and we haven’t had a chance to properly test them… we’re going to do this with some caution but just enough to see us through…” That’s what they were all saying.
And then there was this switch… obviously in the UK the switch came with trying to rush and be the first to approve… In the US it had come with the election, so just around the time of the approvals there was a change in politics… and… the same individuals like Peter Hotez… who had been actually very cynical about these vaccines in public… became vaccine pushers for a different administration.
So again it was very politicised. And… even at that point there wasn’t an intention to vaccinate people that weren’t at risk, and there was still some conversation about levels of risk. But that all seemed to just go out the window…
It wasn’t overnight… I remember this very, very clearly, because I was in the group talking about what was going to be next, and we were saying, “Well they’re not going to give it to people who are 40, or they’re not going to give it to people who are 30… they’re not going to…” And obviously all the while we’re thinking, “They’re going for the children. They’re going to end up [going] for the children.” And actually… the first comment about vaccinating children was in mid-2020.
I am reminded of the salami tactics discussed in this section of June’s Updates post.
And the way that the authorities and media manipulate the narrative: first deny that something (controversial) is going to be done; then discuss it; then make it policy.
[Craig] And then of course they did. And… honestly… I couldn’t believe that that line got crossed… There had been a crossing of line after line after line… red lines… And then they started vaccinating children and pregnant women… [I was] like, “This is… completely insane. These products are novel technology. They’ve never been used before outside of clinical trials, and you’re trying to inject the whole population for a disease that is not a threat unless you are old and sick.” And then… as we’ve [discussed]… that’s probably because you’re not being treated properly… It was madness…
Early observations
[Craig] And what we saw with the vaccine roll-out was… in December 2020… this massive spike of covid that was simultaneously across the country… We’d been following all the data and looking at all the graphs and sharing what was going on. And what you’d see would be these… little wriggly lines in one area as it increased… and it would be decreasing somewhere else. And there was an organic-ness to how the virus was doing its thing.
And then overnight… just as the vaccine [rolled] out… every single corner of the UK had a spike simultaneously… from Anglesey to the Isle of Wight to the Shetlands… all these places that were out of sync with mainland… they’re all going at once… I’ve never quite worked out how much of that was the vaccine and how much of that was changing the testing… I don’t know which one it was. But that spike was weird.
[Coleshill] Did they change the number of cycles?
With PCR testing — with which, according to its Nobel Prize-winning inventor Kary Mullis, “you can find almost anything in anybody” — an increase in the number of cycles increases the chance of a positive test result.
[Craig] You can do things that would alter test results, but there were lots of different labs doing the testing. So actually you’re reliant on being able to command lots of different labs to do something badly, so I don’t think they would have done that… overnight… but I don’t know what was going on. I’m only looking at what came out…
When that happened we thought, “Well, that’s strange.” So we didn’t say we knew what it was, just that [it] was strange. And… what we then saw was that countries were rolling it out at different times. And every time a country rolled it out, there would be a massive spike in covid. And we literally had headline after headline… “Chile has new spike in covid despite vaccination rate…” “Hungary has spike in covid despite high vaccination rates…” It became a running joke, this same phrase being used again and again every time a country started to push the vaccines.
And so we thought… “That’s also strange.” And then… within those first few months there [was] lots of work done to try and show how effective they were. So Public Health England as it was then, and SAGE and other researchers, were gathering data and looking at what was happening in the early roll-out. And what was happening is that in the first two weeks after the people were injected, their risk of covid was through the roof. So you’d get an injection, and instead of it protecting you, you’d be at higher risk for a temporary period, and you’d be sick, and you’d be flooding into the hospitals. And they were trying to get their head around it and writing about it in a very honest way.
I think they were surprised by this result, and they were saying “Well, what is it? Is it people turning up at vaccination centres and catching it there, having been shielding?” It wasn’t that. “Is it people partying because they’ve let their guard down now they’re vaccinated?” This was during lockdown. [And] it was happening in care homes which were heavily locked down. It wasn’t that. “Is it because people are actually coming to hospital with vaccine side-effects and it’s being misdiagnosed?” It wasn’t that…
The immune system after injection
[Craig] It was because, when you inject people with these jabs, they cause cells around your body to turn into spike factories and make the spike protein... And your immune system goes and attacks those cells and kills them, which is problematic in itself, but it also means your immune system is incredibly busy. And… on day 2 after injection there is a massive drop in white blood cells in your blood to… undetectable levels in some cases.
[Coleshill] Undetectable?
[Craig] Yes…
[Interviewer] And those are the [cells] that kill the viruses… deal with any diseases. They are your protectors. So all your security is gone...
[Craig] Yes. You’ve just been denuded of your immune system in your blood… When you’re breathing in these viruses it’s the mucous layer in your lungs… the immunity in your lung is what’s critical, not the immunity in your blood, which is why the vaccines don’t really do anything [to stop covid]. But if you’re hammering the body like that then you are making people sick, and when you’re sick you’re more susceptible to having a viral infection.
And so… what we saw was there more infections and more covid deaths in that period. And… the data [on that] was everywhere… It was in the clinical trials as well. There was this… very high risk early on, but afterwards people who had been infected in that two-week period were then immune from that variant.
So you were… in one of two groups: you were either never going to have a problem with that particular virus because you were immune to it anyway… that was what most people were… Any one wave is only going to… be a problem for about 10% of the population… the rest of us are just bystanders…
Or you were going to get sick at some point during the wave, but your infection has been made early because you got injected. And then after you’ve had that infection, you’re immune.
So what they were doing was ignoring that two-week period when everybody was sick and dying, and then looking afterwards and saying, “Look at this… nobody’s getting sick after these vaccines… because we’re only looking at the period two weeks afterwards…” And they weren’t… And the unvaccinated people would carry on in the trajectory they always would have had, and they could compare the two and say [the vaccine is] 90% effective.
And it looked like that in the data, but it’s an entire illusion based on what happened in that two-week period at the beginning… All you’ve done is made the same people have their cases earlier, and then ignored it and then looked later on and shown the mirage of immunity…
Further related discussion on this can be found in this post featuring Clare Craig’s talk at the Scottish People Covid Inquiry:
![[SPCI-9] "We were told... a story of a lethal virus, a story that only vaccines could save us, a story where vaccines were safe and effective and rigorously tested. But what if that story was wrong?"](https://substackcdn.com/image/fetch/$s_!T0oV!,w_140,h_140,c_fill,f_webp,q_auto:good,fl_progressive:steep,g_auto/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F3b9a0bfd-afd9-4c58-877e-41a3faef29dc_1440x1168.png)
[Coleshill] Because they weren’t counting anything that happened with jabs up to two weeks after the jab…
[Craig] And that wasn’t just in the trials… That was in all of the studies… [in] every single study they would say “Oh well, you see… vaccines… they can’t do anything for two weeks because it takes that long to get an immune response, so we can ignore the first two weeks and then measure it after that.” And the same people making that argument are the people who will tell you, “Oh yes, vaccines… they can only cause side-effects in two weeks, and anything that happens after that’s not related to the vaccine.” There’s something wrong with how these people think…
Quite.
And surely it doesn’t take any expertise at all to see that counting people as “unvaccinated” for (say) the first two weeks after injection is fraudulent?
The many harms of the covid injections
Problems in cells throughout the body
[Coleshill] So what were the harms of the jab, beyond reducing the white blood cells… because [there are] loads on the list… People talk about Bell’s palsy, myocarditis, pericarditis turbo cancer… VAIDS… nerve issues…
[Craig] I feel like I have to address all the ones you’ve just named there, because people are going to think… if I… summarise it all… they’re going to think I’ve covered all of that, and I think some of that is maybe not as evidenced as others…
The big problem with the safety of these vaccines is that, as I’ve described, they… cause problems in cells throughout the body. If you start killing off cells in multiple organs, some people, who’ve got an organ that’s not brilliant… some underlying problem in their kidney say… that they might never have known they’ve had, because they’ve got enough healthy cells to compensate… [if] you go and wipe out some of their healthy cells… they’ll get this kidney problem they otherwise might never have had, or otherwise might have presented years later…
By just killing cells you can end up with conditions in all sorts of organ systems, and each of those conditions is going to get a different diagnostic label… and, for any one of those conditions, they’ll say “Well, overall it hasn’t changed much… There’s no [statistically] significant rise…” because you’ve diluted that overall impact across thousands of diagnostic categories…
Then you’ve got the… autoimmune mechanism, which is true really for all vaccines… If you are teaching the immune system a new trick, as it were, it can backfire, and you can end up with certain people having an immune system that then attacks self. And of course there’s a bit of overlap there, because with most vaccines that is purely an immune misdirection, but, with these [novel technology covid] vaccines, because… your self cells are looking foreign, you can get autoimmune-like illnesses because your body’s responding in a healthy way to foreign-looking cells that have come in under the radar. So there’s autoimmune-type diseases.
And then you’ve got the blood clots and the myocarditis… the ones they’ve admitted to in a big way... If you look at… the list of what’s been admitted to… it’s actually really, really long, but it’s never really been in the mainstream media… Bell’s palsy… transverse myelitis… there’s all sorts of stuff that’s on that list… But the ones that got attention are ones where the background rate of those conditions is… teeny tiny…
For anyone still in any doubt as to the extent of the damage from the covid injections, try searching Google Scholar for “covid vaccination XXX”, where XXX is (for example):
Or if you prefer more technical terms, try (for example):
And keep scrolling and clicking through the results. There are literally thousands of papers. And of course only a relatively small proportion of cases end up being reported in the scientific literature.
So… they’ve said “Well, we’ve got a signal here” because they have multiple times what you’d expect to see in the background.” And ultimately that is the level at which we’re able to definitely detect things. But we have systems in place which have been called out historically as well… where the level of evidence that you need to say we’ve got a safety signal is just far too high. They want 95% statistical certainty before saying that [something] was actually a problem caused by a vaccine… That is not how you treat safety in any other walk of life at all. In any other walk of life you’re like, “Well, 50/50 it’s the vaccine. I think we got a problem guys…” That’s not good enough. They want 95%. If it’s 94%... it’s not the vaccine… It’s a crazy approach to take with regard to safety…
[Coleshill] When you take someone to court, it’s on the balance of probabilities if it’s a civil action isn’t it… a 50/50…
[Craig] But… if you’re talking about people’s health it shouldn’t even be 50/50. I’m of the view that if you’ve got a signal that’s much lower than that, and it’s a concern that it might be causing serious health damage, you take a precautionary approach and you say, “Look… we don’t want to cause harm… First do no harm… that’s one of the basic medical ethical principles.” And we do not do that for vaccine safety… or drug safety generally, actually. We look at these tiny conditions that are increased multiple-fold and we’ll say, “Well that’s a problem”, and we’ll ignore all of these things that have got quieter signals. Although… in some of the results there were absolutely bigger signals than myocarditis.
There was an analysis of the American data. There were… 770 diagnoses where the rate of reporting was disproportionate to other conditions… If you’ve just got a general rise in reporting across the board then it should be increased at a similar rate across the board… You can say well we’re noticing this much of this disease but look how much of this one we’ve got. And you compare them and say, “Well this is obviously something going on…”
[Coleshill] Something’s happened… there’s some external factor that’s come in and caused this…
[Craig] All you’re saying really is [that] doctors with concerns are reporting this condition disproportionately… So let’s look at that… And there were 770 that were disproportionate, and of those there were 500 that had a higher disproportionate reporting rate than myocarditis… That’s also insane. There were real problems with these drugs.
Problems with regulators
[Craig] But what we had was regulators who had this belief that they were doing the greater good… The… drug regulatory system really took shape after the thalidomide scandal of the 60s, where pregnant women were taking a drug for nausea and having babies that had no limbs…
[Coleshill] “Safe and effective”…
[Craig] That’s how they marketed it. That was the slogan…
I am reminded of this 2015 Sunday Times article (link — the original Sunday Times article is behind a paywall) which notes that, “When the thalidomide scandal erupted in 1961, the drug was soon banned. Yet pregnant women in Spain continued taking it until the 1980s — and the authorities refuse to accept responsibility”:

And also this article relating to a dispute in the 1970s between the UK government and The Sunday Times, which notes, among other things that thalidomide prescriptions started in 1958.
[Craig] And what’s tricky about all drug harm is that it’s not every single time. If every single pregnant woman who’d taken that drug had had a damaged baby, it would have been really easy to spot, but… drug harm doesn’t work like that. There’s a proportion that have the problem, so you have to be very carefully observing it to see the proportion…
Then you have drug regulators formed or given more power to keep people safe. And that’s what was it was all about in the 60s… “You guys need to keep the public safe.” And then somewhere along the line has crept in this idea that they should assess drugs based on a balance of risk and benefit. And as soon as you’re doing a balance of risk and benefit at a population level, you can excuse all sorts of harm. And that’s what they’ve done [particularly in the context of covid]. They’ve seen the harm. There’s half a million Yellow Card reports in the UK for these drugs, and they’ve said, “Well, benefit outweighs the risk.”
For more on the Yellow Card reports, see e.g. this post in a series featuring the People’s Vaccine Inquiry:
![[VI] Exposing the UK Covid-19 Inquiry (Module 4)](https://substackcdn.com/image/fetch/$s_!q6No!,w_140,h_140,c_fill,f_webp,q_auto:good,fl_progressive:steep,g_auto/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2Fcc2a63be-6f27-4349-a7c7-d5cc00b63aae_894x898.png)
It is again important to bear in mind here that the UK regulator, the MHRA, receives 86% of its funding from the industry that profits from the products supposedly being regulated.
[Craig] They should not be allowed to say that. That’s clearly terrible for public health, that you’ve got a regulator that can ignore harm because they can pretend they saved lives. And it was pretending, because these drugs didn’t work… We could go there next if you like…
Damage to the heart
[Coleshill] They didn’t work… I’m interested to know how many people they’ve killed and how many people they’ve harmed, because I believe they did tests on the heart, and when your heart is damaged it gives out a certain hormone or signal…
[Clare Craig] You’re not wrong. When you damage the heart, the heart cells that die can release an enzyme into the blood, and you can detect that enzyme in a simple blood test. And it matters because heart cells don’t repair. So if you lose your heart cells, that’s it for the rest of your life. You’ll end up with a scar in your heart where those heart cells were. And this didn’t really happen until boosters were being given… Around that time teenagers were getting second doses, and there were [several] big studies where they did this… four studies…
In Thailand they looked at ECGs of the heart, and blood tests in teenage boys getting a second dose. And 3% of them had a rise in this enzyme after their dose, which is a huge number… What I was saying about how most people are not sickened by drugs that cause harm… most of these boys didn’t have a rise… But3% is far too high if you are giving this to healthy teenagers who do not need it. So that’s the problem. It’s not like everybody’s going to die. [But] it’s 3% of people [that] were harmed, and that’s a massive number… You cannot justify harming 3% of teenagers. That should never have happened.
Such observations are consistent with multiple other indicators, such as the rise in the number of the most serious ambulance calls from early 2021 (p17 here):

And e.g. Scottish mountain rescue callouts (NB Twitter/X seems to have configured that link so that only people logged in can see the post):

And e.g. this recent data from Norway:
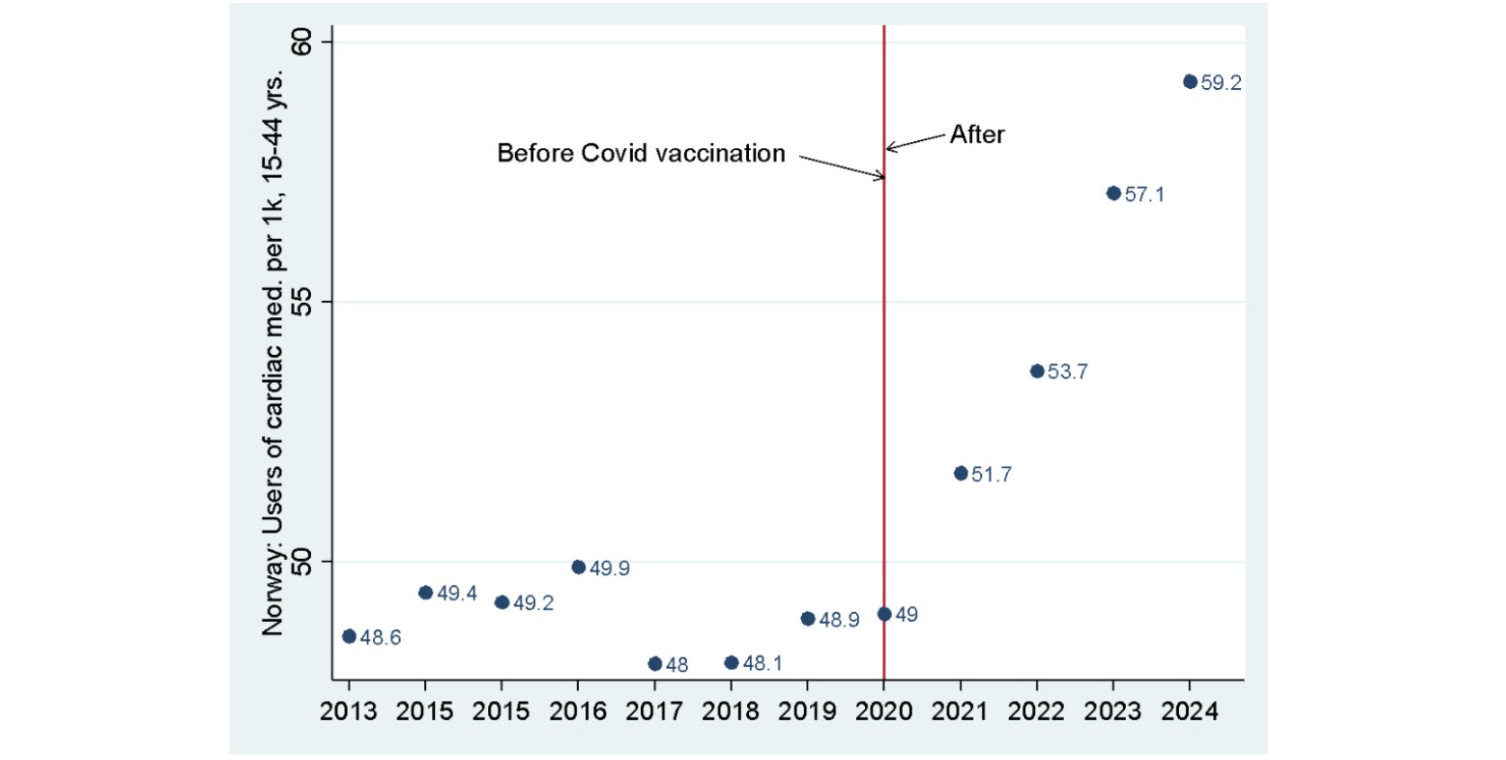
From Jarle Aarstad, professor at the HVL Business School, Western Norway University of Applied Sciences, Bergen, Norway…
“New statistics from the Norwegian Institute of Public Health on the use of cardiac medication (class C, heart and circulatory system) among young people, 15-44 years old, shows an increase of over 20 percent from 2020 to 2024, illustrated in the graph (the y-axis is the number of users per 1000).”
“The increase began in 2021 and coincided with the Covid vaccine rollout to the younger population from the summer of that year. The increase has continued in subsequent years, and the trend does not appear to abate.”
“There was no increase in 2020, which aligns with an Israeli study that found no association between myocarditis and Covid infection before the vaccine rollout. As early as April 2021, the European Medicines Agency (EMA) suspected that the Covid vaccine could cause heart problems, but Pfizer/[BioNTech] — although the vaccine had not even been tested against the spread of infection — still decided to approve it for children, 12 years and older.
I have previously pointed out that young people who refused the Covid vaccine made the best choice. I still believe that, and the graph supports my position.
I wonder when the trend will abate…
For more discussion of myocarditis — inflammation of heart muscle — see e.g. this post featuring consultant cardiologist Dr Dean Patterson:
![[IV] Exposing the UK Covid-19 Inquiry (Module 4)](https://substackcdn.com/image/fetch/$s_!kod0!,w_140,h_140,c_fill,f_webp,q_auto:good,fl_progressive:steep,g_auto/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2Fa8dc4773-80b0-4f06-8d0f-e732204866ba_874x882.png)
[Coleshill] And this is just one of 700 different things… so that 3%... it’s just one of 700 different things. So you can stack all of them on top of each other…
[Craig] And you get to a bigger percentage… There were some other studies that replicated that, including in a middle-aged population of university workers… including in women. So it was not just this teenage boy problem. But what that showed was that this myocarditis in the hospital… in terrible pain… being diagnosed… was a tip of an iceberg of heart damage. The heart damage isn’t always as bad as “I need to go to hospital”, but the heart’s still been damaged underneath and it leaves a vulnerability.
[Coleshill] So later down the road… let’s say they’re in their 40s… You wouldn’t necessarily expect someone to die of a heart attack in their 40s, but they would be more vulnerable, and you might see earlier deaths from heart attacks much younger than you’d expect in these boys…
[Craig] Yes, that’s exactly the right point. And we’ve not been doing enough postmortems, but there are postmortems from around the world that have been reported where they’ve shown either multiple focuses of scarring in the heart muscle or around the vessels of the heart. It often seems to be arising around the vessels which is obviously how this drug’s getting in… you see inflammation, you see those white blood cells that are all attracted in around these vessels where the inflammation is.
And that has a two-fold meaning… On the one hand you’ve got damage to the muscle of the heart… we know that, and that can leave scarring and that can leave a risk of a sudden cardiac death, because the heart is an electrical organ, and if you’ve got scarring that’s a short circuit. And at any point in the future you might get a short circuit and a heart attack and die.
But you’ve also got inflammation in the vessels. And we know this because [with] the mRNA drugs… people were told, “It’s injected into your muscle and it stays there.” And that was so not true. They knew the lipid nanoparticles went everywhere, because they were designed to… that’s what they’re for.
The harms from the so-called covid vaccines were both predictable and predicted. See e.g. this post featuring an explanation from a former Pfizer Chief Scientist:

[Craig] But also Moderna has since done a study where they’ve admitted that only 2% [of the lipid nanoparticles] go into the muscle cells… so you’ve got 98% [going somewhere else in the body]…Where are they going? They’re in your blood supply. So it’s your [blood] vessels that are going to be under stress because that’s where this drug is. It’s circulating around your body and… going into the cells that line the blood vessels… the endothelial cells.
And [if] they start producing spike, and your immune system kills them… that’s a clotting risk, because you need these cells to stop clots… Your blood is is designed to clot, and it will clot wherever there isn’t something saying, “Don’t clot.” And those cells are busy all of the time [sending chemical signals] saying, “Don’t clot here. Don’t clot here.” [And if] you kill them, you’re going to clot…
When you talk about heart disease and heart attacks generally, the vast majority are caused by narrowing and disease in the coronary artery vessel walls. And so if you’ve added in inflammation into these vessel walls of the [coronary arteries] then you’re going to get that disease… You’re going to get atherosclerosis in your vessel walls, and that’s going to cause a higher heart attack risk… that’s the theory…
In practice, that’s exactly what we’ve seen. We’ve seen cardiac deaths and cardiac presentations… even in young people… go up after 2021. And the key data point is in South Australia…. they had [only] a thousand covid diagnoses by the end of 2021… that was it… And yet they saw this spike in young people with cardiac problems turning up at the emergency departments.
And it peaks in November of 2021. And then Omicron comes in December and shoots up in January, and they’ve had covid since. But that… heart problem [occurred] prior to covid in that part of the world.
How many people have died from the injections?
[Coleshill] So, looking at the overall harm that’s been caused… how many people do you think have been killed by these jabs… It’s a massive question. You’ve got these 700 different factors… different metrics of harm, so is it even possible? Could you give me a scale…? Is it hundreds, thousands, millions, tens of millions…
[Craig] This is a really important question, and one that I shouldn’t dodge, but I’m going to because there are too many factors to put into the equation. For example, lockdowns killed people, and lockdowns continued to kill people after they were over.
We saw in autumn of 2020 too many cardiac deaths of people aged in their 40s, particularly men… but nevertheless the stress of lockdown and the fear propaganda is something that we know would cause cardiac death because it’s… evidence-based that kind of psychological stress causes cardiac disease. And there you go… they started dying before the vaccines.
You’ve got to try and subtract the fear propaganda deaths from the total excess deaths, and I don’t know how you do that… That’s a difficult sum to do… It becomes quite uncertain. If you wanted to do [the analysis] properly, you would want to have really good data on what products were given in different places at different times, and proper datasets of who had what when… and the follow-up of them… And you’d also want to know what their background health status was because you can’t do this sum without background health status.
And when you’re getting into older age groups it’s difficult because you’ve got a lot of background deaths. And so the… additional deaths get drowned out. When you go to younger age groups you’ve got a different problem which is that younger people tend not to die, which is great. But the people who do die young… about half of them know it’s coming… Half of them are sudden deaths and half of them are expected deaths. And those people who are expected to die almost all got vaccinated. So you’ve got a bias there in the mortality data… that you’re already more likely to die if you’re vaccinated. And so that becomes very hard to unpick… data around covid was everywhere… we were just completely swamped with it in a way that is actually almost unbelievable… [and] I don’t believe all of… that data was collected in the way they claimed, because it would have been impossible to… but data around the vaccines is just hidden…
At one point, the UK was really leading in terms of transparency around data, and UKHSA was publishing detailed data on a weekly basis by vaccination status… who had what… And it started to go really horribly south for the vaccinated, and they just pulled the data… That’s really dishonest, isn’t it.
But of course… strategically it makes sense because… when we’ve got no data to analyse there’s no news to be told. If you’ve got a constant stream of “Well, this has happened now, and then this has happened”… we can make news from it. But there’s no news to tell when there’s nothing [reported]… It’s just silence… So we have to keep [reminding people that] they hid the data… that’s not really news anymore…
[Coleshill] Until the data is eventually given…
[Craig] We’re fighting for it … and we have had some data out of some countries. And I think… maybe in the end we will get more data…
I am reminded of these posts, featuring analysis of official data in the UK:

And this analysis of life insurance data from the US:

[Craig] But just going back to the point about the covid data… For example, in the UK there’s a lot of data published about intensive care, and they made out they knew exactly what was going on in every intensive care unit in the country, down to the vaccination status of all those people, and when they were vaccinated. And they presented all this data.
But in reality there are big problems with it. One is that you can’t guess the size of any population. You can measure the size of how many people you put a needle into. But when you’re saying, “How many people did we not put a needle [into]… we’ve got to guess how many people there were altogether, and then subtract how many are vaccinated. So that’s always a bit of an estimate.
And they were using ONS estimates which were ridiculously small, to the extent that there were more people who were vaccinated in certain age groups in regions of the country than the ONS said existed… so you had negative unvaccinated people!
But when you’ve got a tiny number of unvaccinated people and you’re saying, “Well, look how many people per 10,000 are on intensive care with covid” and you’re saying, “Well, there were only two unvaccinated people” then you can create a huge rate and say, “Oh, this is awful.”
A positive result from a test with no false positive rate was enough to define a death as being “with covid”.
Incidentally, the link to the written answer to a question in Parliament in October 2020, where it was disclosed that “the United Kingdom operational false positive rate [for covid PCR testing] is unknown” now gives this message:
“Something has gone wrong”
In more ways than one.
[Clare] But, worse than that, they were including people whose data was “unknown” in their “unvaccinated” groupings, which is also what was happening in America. And in America the systems really are not connected at all. So in… most situations the patients in America had an unknown vaccination status, and those unknowns were called “unvaccinated” and they had a “pandemic of the unvaccinated” which was really a pandemic of “We don’t know what status people have”… It was… ridiculous.
[Interviewer] I think one of the reasons people really want to suss this out is because they want to know the scale of the crime, because it’s the possibility that it could be in either the tens of millions or hundreds of millions of people who will either die from it or will have their lives significantly shortened at some point later. So it’s whether we’re going to see, like we said with those boys, people dying off 20… 30… 40 years before they should because their heart’s been weakened and they have a heart attack, or something happens with their kidney, or something happens with something else…
[Craig] First of all, there is an upper bound on the deaths because you can say, “Well, if there had been hundreds of thousands of deaths in the UK, say, you’d see it in the total…” I’m just giving that as an example… So there is an upper bound on how many deaths there could have been, because you can say, “Well, this is within the bounds of the total number of deaths.”
In terms of illness it’s much, much harder, because if you’ve got somebody dying… and the time between when they had the drug and their death is big, and you haven’t had a postmortem — and even if you did have a postmortem you can’t prove that the drug had a role to play especially, because we’re not doing any of the tests that might help with that — it becomes it’s difficult to prove [a link]…
Then you’re back to the data… and then with the data you’re like, “Well, what else has changed over that period of time? Well, we had the stress from lockdown… we had whatever else…” And… that’s really, really hard now to say, “Well, if you’d been in my generation you would have died at this rate, but you’re younger… it’s this rate…” How do you know?
How many people became sick after being injected?
[Coleshill] So how many people would you say actually got sick overall?
[Craig] I think that’s a really key point. And that is something that we can put a number on, because what we’ve seen is that the number of people who are working age and unable to work because of long-term sickness… which is a question the ONS asks in surveys… has gone up from Spring 2021. We had a lot of covid without that changing… [the number of people unable to work] just wiggled around the way it normally does…
And then from Spring 2021, when the working age population started to be injected, that [number] just went up and up and up… and it ended up around 2% of working aged people – 1 in 50 working age people… 800,000 of them – unable to work. [And] that again is a tip of an iceberg, because obviously you can be sick and still able to work. But that’s a big problem. That’s a huge number, and it’s way, way bigger than any estimate of what “long covid” has caused, whatever [that] might be.
See e.g. this post:

[Craig] But I don’t really dismiss [long covid]… I think… people who’ve had viruses do get long-term problems. That was always the case, and absolutely people have had problems after covid. And that was the case before vaccines. But ultimately, no matter how much you try and exaggerate the number, it cannot account for all of those people who are sick. And the same happened in the USA…
Here is a chart of official US Bureau of Labor Statistics disability data showing a marked rise in the population with a disability since early 2021:

NB the numbers on the y-axis refer to thousands of persons.
[Craig] But what’s interesting… and I must go and dig into this data because I haven’t done this yet… our [UK] levels seem to plateau mid-2023… We stop jabbing the working age population, and that figure stops rising. But the US just produced their latest data, and it’s still going up there, because they’re still vaccinating anyone that wants to go to college or anyone who… hasn’t figured it out yet… There’s still a lot of vaccinating going on in a country that has always been… big… into vaccines. So they’re still going for it, quite a lot of [Americans]…
That is the end of part 2. The final part of the podcast — featured in part 3 — includes discussion on other vaccines (including a horrific hypothesis for much of the childhood mortality in the 1800s), recent developments in the US, judicial consequences for covid era crimes, and autism.

Related:


Unexpected Turns homepage
The most-read articles can be found here
I had to log in to Twitter/X to access that link